Involuntary psychiatric care
Involuntary psychiatric care is an intrusive and ethically complex form of care where the evidence base is still limited. John Wallert’s team studies risks, interventions and how involuntary care can be followed up and evaluated.
Research on risk, follow-up and effects
Involuntary psychiatric care may be necessary in severe psychiatric conditions and acute crises, when the need for care is considered indispensable but the person opposes voluntary care. At the same time, this form of care is resource-intensive and involves major restrictions on patient autonomy. It requires not only substantial clinical resources, but also extensive legal processes.
Wallert’s modelling team conducts research that strengthens knowledge about involuntary psychiatric care through both predictive and causal studies. The research includes studying risks after discharge, developing decision support for follow-up, mapping the use of coercive measures, and analysing how involuntary care can be evaluated in an ethically and methodologically robust way.
In a national register study, the team has investigated suicide risk after discharge from involuntary psychiatric care in Sweden. The results show that suicide risk is elevated after discharge, particularly shortly after the care episode, and that the risk varies between patient groups and diagnoses. This knowledge can contribute to better risk assessment, more targeted follow-up and more precise interventions after discharge.
The aim is to increase knowledge about which patients are at greatest risk of adverse outcomes, how care can become more equitable and safe, and which study designs can provide better answers about the effects of involuntary psychiatric care.
Risk calculator for follow-up after discharge
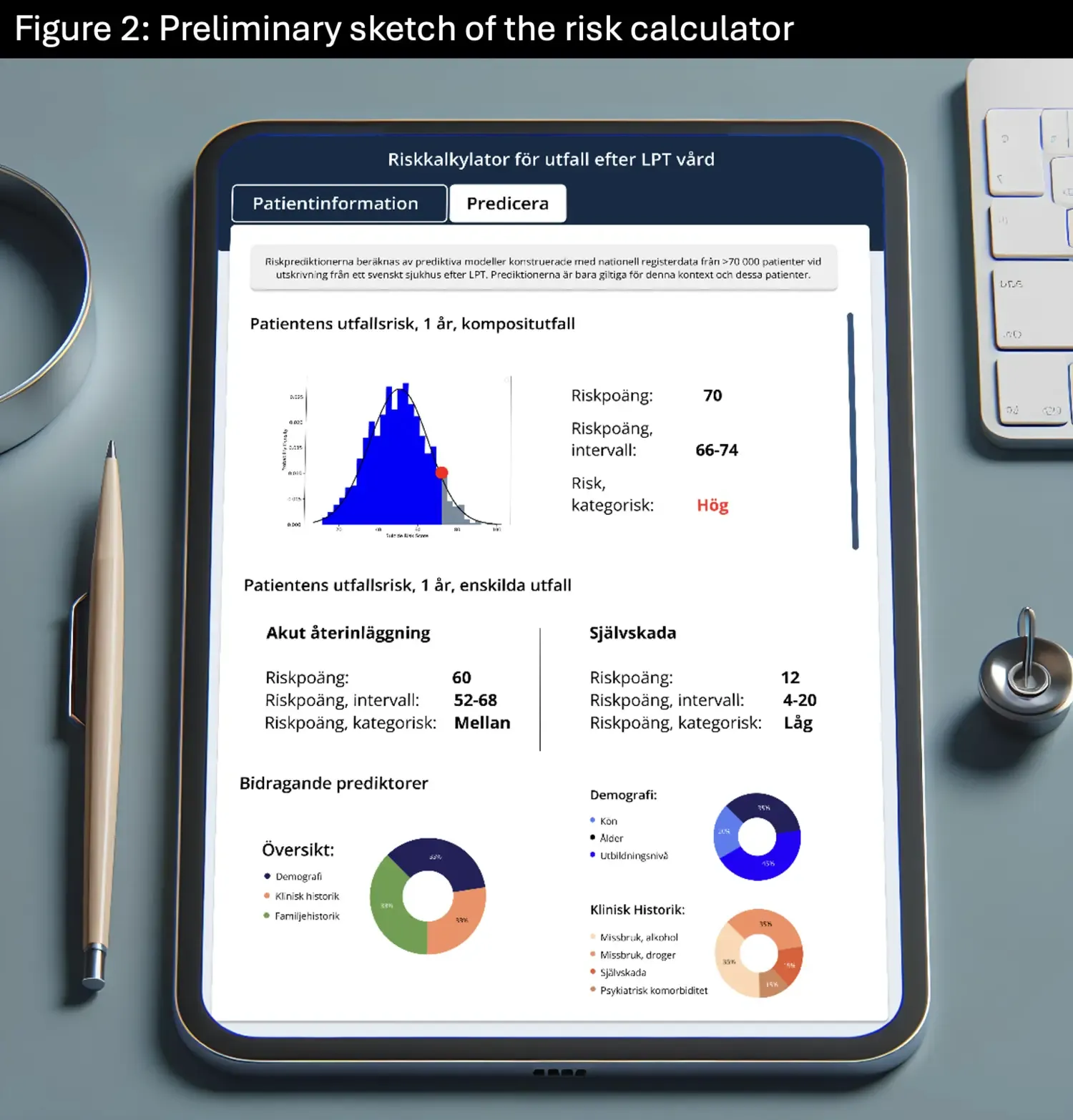
The team is developing a population-based risk calculator for adverse outcomes after involuntary psychiatric care. The aim is to develop a decision support tool that can be used at discharge and when planning follow-up care.
The risk calculator will estimate the risk of serious adverse outcomes after discharge, such as suicide, self-harm leading to hospital care, or acute psychiatric readmission. The project is based on national register data on individuals who have received involuntary psychiatric care and uses the largest dataset of its kind. The project combines traditional statistics, machine learning and clinical knowledge.
The development also includes interviews and focus groups with physicians and people with lived experience of involuntary psychiatric care. The aim is to examine usability, acceptance and ethical aspects, as co-creation is central to ensuring that the decision support tool is relevant and useful in everyday clinical practice.
In the long term, the decision support tool may help ensure that patients at high risk receive more tailored follow-up after discharge.
Coercive measures during care
Part of the research concerns coercive measures used during involuntary psychiatric care: mechanical restraint, forced medication and seclusion. The team studies how these measures are used, how their use varies between patient groups and how coercive measures can be measured reliably in register data.
The work involves both describing the occurrence of coercive measures and validating the variables used to study them. This is important because more reliable data can provide better knowledge about which patients are at higher risk of being subjected to coercive measures and how care can be developed to become more equitable, safe and legally secure.
By combining register data with clinical knowledge, the team aims to contribute to a more robust evidence base on coercive measures during care. In the long term, the research can be used to identify preventive interventions and improve the follow-up of involuntary psychiatric care.
Ethics and methodological study design
Involuntary psychiatric care is difficult to study because it is often ethically problematic to randomise patients to involuntary or voluntary care. At the same time, more knowledge is needed about the effects of involuntary care, as this form of care involves major restrictions on patients’ freedom and autonomy.
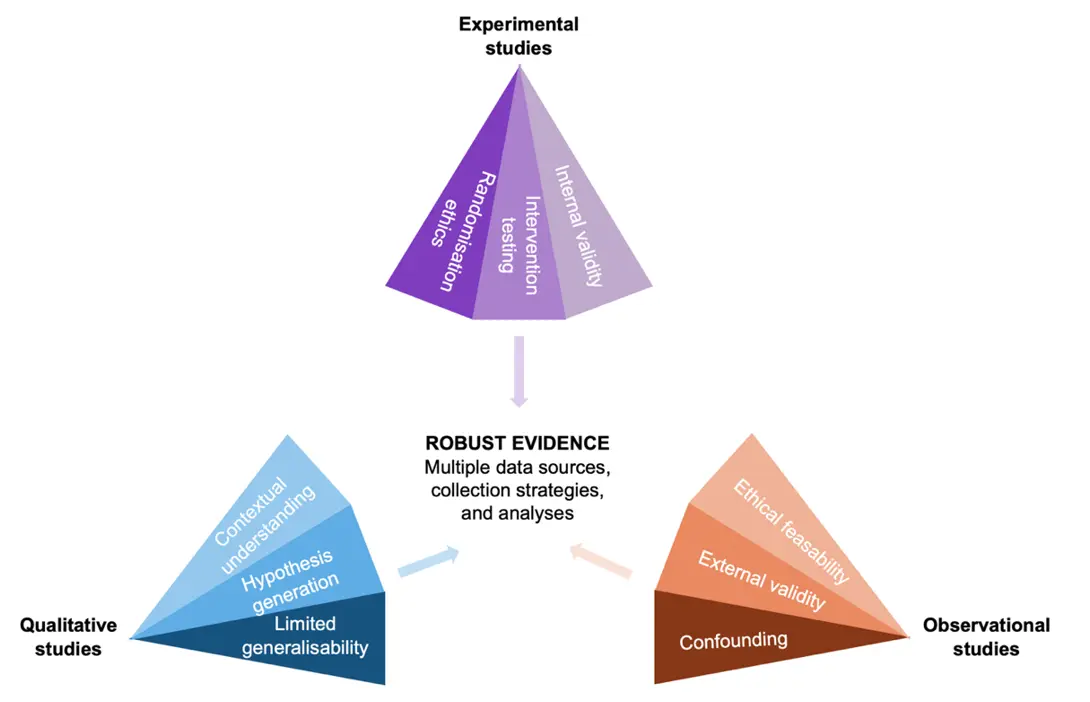
The team is therefore developing an ethical and methodological framework for how involuntary care can be evaluated. An important starting point is that different types of studies need to complement each other. Register studies can identify patterns and risks in large populations, qualitative studies can provide knowledge about the experiences of patients and healthcare staff, and experimental or quasi-experimental designs can contribute better knowledge about cause and effect.
Together, these approaches can provide a more robust evidence base for the future of involuntary psychiatric care.

Funders
The research is supported by Forte, the Swedish Research Council, Region Stockholm and CIMED.
Published and ongoing articles
Grossmann, L., Johansson, F., Fazel, S., Kuja-Halkola, R., Bråstad, B., Mataix-Cols, D., Fernández de la Cruz, L., Runeson, B., Lichtenstein, P., Chang, Z., Larsson, H., Brikell, I., D’Onofrio, B., Pingel, R., Rück, C., & Wallert, J. (2026). Suicide after involuntary psychiatric care: a nationwide cohort study in Sweden. The Lancet Regional Health – Europe, 60, 101504. https://doi.org/10.1016/j.lanepe.2025.101504
Rück, C., Grossmann, L., Johnson-Singh, C. M., Gubi, E., Brenner, P., Gardner, R. M., Wallert, J., & Johansson, F. Absolute and relative risk of mechanical restraint, forced medication, and seclusion during involuntary psychiatric hospitalisation: a population-wide cohort study. Preprint/manuscript.
Grossmann, L., Jonsson, F., Johansson, F., Dahlin, M., Brenner, P., Rück, C., Sjöstrand, M., & Wallert, J. Involuntary psychiatric care should be evaluated: towards an ethical methodological framework. Manuscript.
Grossmann, L., Johansson, F., Rück, C., & Wallert, J. Risk indicators for suicide after involuntary psychiatric care. Preregistration. Open Science Framework. https://osf.io/nyftu/
Grossmann, L., Johansson, F., Flygare, O., Axelsson, E., Turesson, M., Rück, C., & Wallert, J. Involuntary Psychiatric Care in Relation to Clinical and Sociodemographic Outcomes in Adult Patients: A Systematic Review. Preregistration, Open Science Framework. https://osf.io/z7w2n/
Grossmann, L., Johansson, F., Rück, C., & Wallert, J. Suicide in the compulsory mental care population in Sweden: a descriptive nationwide registry study. Preregistration, Open Science Framework. https://osf.io/k56np/