The Northern Swedish Cohort
The Northern Swedish Cohort is performed in collaboration between Karolinska Institutet (Unit for Occupational Medicine at the Institute of Environmental Medicine (IMM) and Umeå University (Department of Epidemiology and Global Health).
We welcome scientific collaboration around the cohort. Ethical approval is a prerequisite. Contact the PI of the cohort, Anne Hammarström for further discussion.
Ann Hammarström
Principal investigatorThe start of the study
The Northern Swedish Cohort was started by Anne Hammarström (principle investigator, PI) in collaboration with Urban Janlert and other researchers within the field of social medicine (Ragnar Berfenstam, Finn Diderichsen, Töres Theorell, Lars H Gustafsson, Claes Sundelin, Gustav Jonsson). At that time the PI was a newly qualified registered medical doctor and was searching for a PhD project. An older colleague advised us to start a longitudinal study, which could be the database for our future research.
The background to the study was the relatively high unemployment rate among young people in Sweden at the beginning of the 1980s. While some studies were available about the health consequences of unemployment in the adult population, there was a lack of research about possible health consequences of youth unemployment. Thus, we decided to perform a longitudinal study of a cohort of school leavers. The chosen setting was Northern Sweden, as the highest levels of both youth and adult unemployment were found in that part of Sweden. In fact, unemployment had been endemic in this part of Sweden for a long time. The county capital of Norrbotten – Luleå – was chosen as this is a typical middle-sized, industrial town which was comparable to Sweden as a whole with regard to important socio-demographic background data such as labour market structure, percentage of foreign-born, housing, divorce rate and socioeconomic status.
Initially, we planned to follow-up the cohort after two and after five years. However, after the first five years the study had attracted the interest of the scientific community and of policy makers, and thus there was a request for new follow-ups.
Funding agencies
Until the investigation in 1995, the cohort study was funded by the former Delegation for Social Research and the Institute of Social Research. The investigation in 2008 was financed by the Swedish Council for Working Life and Social Research, the National Institute of Public Health, the Swedish Research Council and the County Council of Västerbotten. The latest funder is FORMAS and FORTE.
What does it cover?
The original research topic was to examine the health consequences of youth unemployment. What are the social and medical consequences of youth unemployment? Which young people become unemployed? What are the effects of labour market measures?
The possible consequences of youth unemployment for health in adult age was also the focus of the application for the follow-up in 1995, but this time the research questions were broadened to include analyses of the life course and trade cycle occupation. The research questions focused on the possible health consequences of unemployment and whether these relations were influenced by occupation, length of unemployment, age, gender and socioeconomic status.
The investigation in 2008 has included four major projects. One has a broad focus on the health consequences of the structural transformations of the labour market that were initiated during the 1990s. The transformation led to increased flexibility on the labour market, with more temporary employment and higher rates of unemployment. The aim of the study was to analyse the association between insecure labour market attachment and health. The hypothesis was that the more time in insecure labour market attachment, the poorer is the health status, and that movements from the periphery to the centre of the labour market will lead to improved health. Our theoretical premise was that insecurity, inadequate possibility of development and lack of decision latitude in work can lead to stress reactions, which in turn manifest themselves in deteriorated health behaviour and health status (self-reported symptoms, depression, blood pressure, cortisol etc.).
The aim of the second project of the follow-up in 2008 is to analyse the importance of gender equality in domestic work for the health status of men and women. One of the main research aims was to analyse whether a higher degree of gender equality in domestic work is related to better health among men and women. The research questions also included the following: Does greater gender equality in domestic work promote improved health behaviour amongst men? Could decreased workload explain the relation between improved gender equality in domestic work and better health among women? Does labour market attachment and socioeconomic status influence the relationship between gender equality in domestic work and health? What is the importance of health-related selection? The second main research area was based on qualitative analyses of the research question: What does gender equality in domestic work mean for the construction of masculinities and femininities in couple relationships and for the experiences of health?
The third project is related to the Barker hypothesis on the foetal origins of adult disease, i.e. that adaptation in utero to unfavourable conditions will affect health in adult life. Our point of departure was that a methodological problem in most studies of this hypothesis is the lack of possibilities to analyse intermediate variables between birth and the development of diseases in adult age. The aim of this project is to study whether signs of foetal growth retardation could predict biological risk factors for cardiovascular diseases in adult age, even after controlling for a life-course exposure, i.e. the accumulation of adverse life experiences from childhood to adulthood.
The fourth project focuses on modifiable risk factors (social, psychological, biological) during the life course for metabolic syndrome in adult age. One research question is to explain the excess risk of the metabolic syndrome among women who grow up in unfavourable circumstances. Another research question focuses on explaining the excess risk of the metabolic syndrome in adult age among men as compared to women.
The results from the four research programmes are summarised in Populärversion.
The sample
The cohort consists of all pupils who in 1981 attended, or should have attended, the last year of compulsory school (age 16) in all schools in the municipality of Luleå. The PI visited all 46 classes in the last year of compulsory school in the municipality of Luleå and asked the pupils if they wanted to be part of the longitudinal study. Written information was given to them, as well as to their parents. The local municipality provided lists of all pupils in the last year of compulsory school, and all form teachers were asked whether any pupil had left compulsory school in advance. Those eleven pupils who had left school in advance (for various reasons such as childbirth or school fatigue) were contacted and personally visited by the PI.
The study was preceded by a major effort to anchor the project in the local municipality as well. The PI visited the local education authority, all principals of the nine compulsory schools within the town, all school nurses, all study and careers advisers, the parent-teacher association as well as the pupils’ association. They were all invited to send a representative to a reference group concerning the study, and all of them did except for the trade union. The aim of the reference group was to plan and design the study as well as to get early feedback about the results. The reference group continued its work until the 1986 follow-up had been performed.
The attrition rate was extremely low. Of the total 1083 pupils (506 girls, 577 boys) who were invited, 1080 participated in the baseline investigation. The missing three boys who were invited but did not enter the study were all sons of high-educated parents.
A subsample was made from the cohort, consisting of all participants who were in open unemployment directly after compulsory school (n=13 girls, 15 boys). They all agreed to be part of the study.
All school nurses and form teachers in 1981 as well as all form teachers in 1983 were also part of the sample. None refused to participate.
Follow up
As shown in Figure 1, the cohort has been followed up five times – in 1981 (age 16), 1983 (age 18), 1986 (age 21), 1995 (age 30) and 2008 (age 43). Clinical measurements were performed in 1981, 1986 and 2008. Interviews were performed with key persons – with the school nurses in 1981 and with the form teachers in 1981 and 1983.
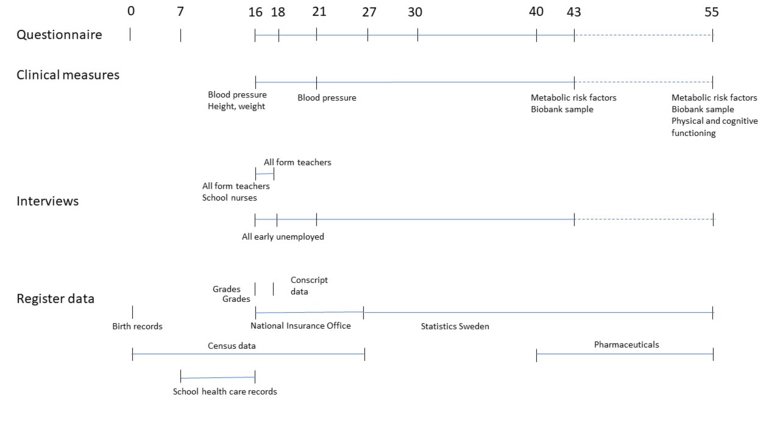
The subsample with early unemployed participants has been followed with personal interviews since autumn 1981. Until now, they have been interviewed on average four times per person. The main topic has been the health consequences of unemployment.
Register data
The following register data has been added to the cohort:
1. Manual record of birth data from participants own birth: height, weight, physical status, malformation, gestational age; data regarding the mother: age, parity, diseases, complications during delivery.
2. Manual record of school, class and (in upper secondary school) also study programme, based on information from each school.
3. Manual record of grades (for each subject from the last year of compulsory school) based on information from the local municipality
4. Manual record of school health data: Measurement of vision, sense of colour, hearing, weight, height, number and diagnosis of visits to the school physician (during the last three years of compulsory school), referrals (instance and diagnosis).
5. The following data have been added from the longitudinal integration database for health insurance and labour market studies (Swedish acronym LISA) at Statistics Sweden for each year between 1992 and 2007: employment, number of employees at one’s workplace, number of sources of income, number of days (gross, net) per year in allowances due to parental leave, temporary parental leave (due to care of sick children), sick-leave, rehabilitation, work injury, preventive sick leave, unemployment and labour market measures (and which type of measures).
6. The following data have been added from the National Social Insurance Office for 1982, 1983, 1985 – annual information about civil status, number of days in parental leave (all data missing for 1984, 1986, 1987). For 1988–1992 the following data have been added: Annual information about civil status, number of days in parental leave, extent (whole, 25%, 50%) for the participant as well as the other parent. For 1988–1992 annual information about the number of days’ sick-leave and extent (whole, 25%, 50%) has also been added.
7. The following data have been added from the longitudinal integration database for health insurance and labour market studies (Swedish acronym LISA) at Statistics Sweden for each cohort participant as well as for all other employees at their workplaces (from 2003 until 2007): sex, age, income, education, type of workplace, number of days (gross, net) per year in allowances due to parental leave, temporary parental leave (due to care of sick children), sick-leave, rehabilitation, work injury and preventive sick leave.
Ethical clearance
The study has been approved by the Regional Ethics Vetting Board in Umeå. A new application has been sent to Etikprövningsmyndigheten.
Overview of data
Measurements
Blood pressure was measured at age 16, 21 and 43 and information on body mass index is available from age 16 (from the school health records), 43 (measured), 21 and 30 (self-reported). The most recent survey at age 43 also comprised a health examination including measurement of waist circumference, and blood sampling after one night’s fast were assessed for total cholesterol, HDL and LDL cholesterol, triglycerides, apolipoprotein A1 and B, fasting glucose and C-reactive protein. The participants also completed a one-day saliva collection (four samples) assessed for salivary cortisol. One blood sample was also stored at the biobank at Umeå University Hospital.
Data from interviews with key persons
The interviews (about each participant) with the school nurses dealt with the presence and severity of eczema and/or allergy, other illness or handicap, number of visits to the school nurse (in the last year of compulsory school), main diagnosis of school nurse visit, taking part in pupils’ well-being meeting.
The teacher interviews (about each participant) in 1981 covered the following items: the behaviour of the class, knowledge about the class, composition, number of years in teaching, gender of the teacher, attitude towards the pupil, the pupil’s intellectual capacity, performance, gross motor ability, fine motor ability, difficulties in reading and writing, speech problems, language problems, Swedish as mother tongue, smoking, alcohol consumption, truancy, absence due to other reasons, Monday absence, knowledge about problems in the family, parental interest in the pupil’s studies, parental attitude to the pupil, prospects for future work and studies, opinion about the pupil, assessment on a six-grade scale of the pupil’s tiredness/alertness, depressiveness/exhilaration, passivity/activity, silence/outspokenness, dependence/independence, aggression/lack of aggression, insecurity/confidence, isolation/extroversion, unpopularity/popularity among students, unpopularity/popularity among teachers.
Interviews (about each pupil) were also performed with the form teachers in 1983 about the class (knowledge about the class, composition, number of years in teaching, gender, attitude towards the pupil) as well as about the pupils: difficulties in reading and writing, dependence/independence, aggression/lack of aggression, ability to concentrate or not, unpopularity/popularity, unhelpful/helpful, knowledge about illness, psychological symptoms, abuse (alcohol, narcotics etc.), criminality, knowledge about parental illness, psychological symptoms, abuse (alcohol, narcotics etc.), prospects for future work.
What is attrition like?
During the 27-year period, 12 participants died. At the 27-year follow-up 94.3% (n =1010) of those still alive of the original cohort (n=1071) continued to participate. Thus, over the 27 years 6,3% of the participants have been lost and about 1% of these is due to premature deaths (see Figure 2).
Among the non-responders there is an overrepresentation of boys (77% among the non-responders compared to 52% among the responders), of individuals with low grade from compulsory school (48% compared to 41%) and of low parental socioeconomic position (57% compared to 53%). A similar patterns is also found among the participants who died during the follow-up. As the attrition rate has been so low it has been possible to study marginal groups as e.g. unemployed, addicts and persons with psychiatric problems.
Summary of findings
Our research on unemployment and health has shown that:
- youth unemployment causes significant health problems (both somatic and psychological) as well as deteriorated health behaviour (such as smoking, alcohol consumption, sexual risk-taking), even after control for possible confounders
- the health consequences of youth unemployment remain to a certain extent in adult age, independent of later unemployment
- among young people, the effects of exposure to unemployment seem to be stronger than those of selection (earlier health status)
- the longer the exposure to unemployment, the worse are the health consequences.
- women are harder hit than men (and young people harder than adults) by the health consequences of unemployment
- transition from unstable labour market position to permanent employment seem to be health-promoting
- recession had little or no impact on the health status of the unemployed young people.
- but recession seemed to have a negative influence on the health situation of young women who worked and studied.
An analysis of the impact of early health/health behaviour on future socioeconomic position showed no such relations. However, even after correction for possible mediating and moderating mechanisms, being overweight at age 16 and at age 21 was related to future working-class position among women only. Our results indicate that overweight girls and young women are exposed to gendered discrimination, which probably occurs in many arenas, based on the norms for female bodies in our society.
One of the theses based on the cohort showed that the social patterning of health was gendered and age-specific depending on the outcome measures. Unfavourable school environment in early years had long-lasting negative influence on later health, health behaviour and socioeconomic position. The thesis supports the notion of accumulation of risk that social inequities in health occur due to the accumulation of multiple adverse circumstances among the lower socioeconomic status throughout their life course.
Our research also shows a negative relationship between being in temporary employment and health status. Important mediators of these effects seem to be low cash margin and job insecurity. Another study with 12 indicators of health showed that exposure to non-permanent employment may affect mental health, whereas the effects on somatic health and health related behaviour are scarce. In fact, job insecurity was more consistently and strongly associated with poor health than non-permanent employment. Moreover, the health effects of non-permanent employment depend on the socioeconomic status of the employees, being more adverse in the less educated.
Another research theme of the cohort has focused on the life-course origins of metabolic health in mid-adulthood. One study showed that social inequities in overweight reflect the cumulative influence of multiple adverse circumstances experienced from adolescence to young adulthood. Underlying pathways to social inequity in overweight differ between men and women. We have examined different socioeconomic life-course models for metabolic outcomes in mid-life. We have found support for the cumulative risk and sensitive period (in adolescence) models for serum lipids and for allostatic load, but that the circadian cortisol regulation, particularly the cortisol awakening response, appears to be mainly related to early socioeconomic circumstances, corresponding to a sensitive period model. We have also demonstrated an association between adolescent socioeconomic status and the metabolic syndrome in mid-adulthood in women, independently of BMI and blood pressure in adolescence and young adulthood and of socioeconomic status and health behaviours in adulthood. These findings thus suggest other pathways than an early impact of socioeconomic disadvantage on metabolic systems which tracks into adulthood; this will be explored in future manuscripts from the cohort.
We have also examined the importance of birth weight for circadian cortisol regulation and for serum lipids. For cortisol levels, we found that across the normal birth weight spectrum there is a positive association between birth weight and cortisol levels, particularly in the evening, but also high levels in those born preterm or of low birth weight. Of a range of serum lipids (total cholesterol, LDL and HDL cholesterol triglycerides, and circulating levels of apolipoprotein A1 and B) examined, we found support only for the foetal origins hypothesis for triglycerides in women, albeit independently of the life-course accumulation of unfavourable social exposures (socioeconomic status and adversities). Overall, social exposures displayed stronger relationships to lipids than did birth weight.
An analysis of the importance of gender equality in the couple relationship showed that perceived gender inequality in couple relationships seems to be an important determinant of psychological distress for both women and men. Also, for women only, taking the whole responsibility for domestic work and for men taking less than half of the responsibility for domestic work was associated with psychological distress.
Main strengths and weaknesses
The main strengths of this study are the extraordinarily high response rate in combination with the long follow-up time. A cohort of school leavers from a middle-sized town has been followed for 27 years. The question of the generalisation of the results from the Northern Swedish Cohort needs to be discussed. The participants have been followed regardless of where they have moved (in Sweden or abroad). The cohort has proven to be comparable to the country as a whole with regard to socio-demographic and socioeconomic factors as well as health status and health behaviour. The cohort is closed, which means that the cohort today is more a homogeneous ethnic group than the Swedish population as a whole.
At the time the cohort was chosen, the sample size was regarded as large. Today the sample size is regarded as relatively small, which is the main limitation of the study. However, it would have been extremely difficult to keep up the high response rate with a larger sample. One important prerequisite for the high response rate has been the close relation between the project leader and the participants – the PI met the participants several times during the follow-up, blood pressure measurements, interviews etc. As of the participants said at the 27-year follow-up: “I never participate in studies but I do in this case because I know you.”
So, would we had done the study differently today? The answer is no and yes. No, we would have devoted all the time we did in order to get a high response rate during a long-term follow-up. And no, it would have been impossible to have personal contact with a much larger sample size. It was good to concentrate on one town – the study has become famous in that town and it was relatively simple to establish support for the study among key persons/groups before it started. We also believe that we initially put heavy emphasis on defining a theoretical point of departure which guided our research questions. The theories we chose are still valid today, and even after 27 years we are satisfied with most questions in the questionnaire. What we lack is more early questions about abuse (physical, psychological, sexual) and social support as well as measures of the positive dimensions of health.
Our growing interest in life-course epidemiology would of course have benefited from starting the study earlier, at birth or at least in grade 1. Also, as our theoretical perspectives have widened, if we had done the study again we would have included questions later added (GHQ, social support etc.) from the beginning as well as questions about childhood and adult abuse, salutogenesis (or other positive aspects of health) as well as social capital. Also, for analyses of biological risk markers we would have stored blood samples from the beginning of the study (preferably at birth).
We would like to give the following teaching points to researchers who want to set up a similar study:
- Be sure to anchor the research among key persons before you start a cohort study.
- Spend time formulating your theoretical premises, which will then guide the questionnaires for a long time.
- Feedback on the results from each follow-up is important in motivating the participants for subsequent participation.